Posts Tagged history
The Lancellotti Discobolus
Posted by Bill Storage in History of Art on June 9, 2026
Engineering meets art history
The Discobolus of Myron is one of the most famous sculptures in the world, despite the fact that it no longer exists.

What you see here are two Roman marble copies of an original Greek bronze, made perhaps four hundred years earlier. As I stand in Palazzo Massimo, looking at the famous Discobolus Lancellotti and the more damaged version to its left, It seems to me that “copy” doesn’t tell the whole story.
How do we know it’s a copy if the original is lost? We don’t. Not really. But a few pieces of evidence support it. Multiple Roman statues survive showing nearly the same composition with variations. Ancient writers, especially Pliny the Elder, mention a famous Discobolus by Myron. From this, scholars infer a lost Greek prototype.
But that inference depends on assumptions. That Roman versions derive from a single famous original. That the literary references correspond to these sculptures. That the similarities are too strong to be coincidence,
and that Roman sculptors were reproducing admired earlier works rather than improvising freely and copying each other.
Reasonable conclusions, but not certain. Classical archaeology, seems to me, often speaks with a certitude that conceals how inferential the whole enterprise is. The “original Myron Discobolus” is a scholarly composite. The original survives as an intellectual reconstruction.
The nearly-complete Discobolus Lancellotti looks so perfect that people instinctively assume it must be the “best” copy. But the fragmentary version beside it in some ways preserves more truthful structural details. In particular, traces of the massive support on the hip show how difficult the pose really was in marble. Bronze could suspend limbs in space. Marble – not as much. The cleaner version partly hides the engineering problem.
The first thing that strikes you about the Discobolus is motion. Or rather, suspended motion. The body is wound tight, almost like a spring under torsion. The torso twists against the hips. The shoulders oppose the legs. We see stored rotational-energy.

But the face remains calm, almost indifferent. Modern athletes grimace and strain. Our culture likes that. Greek classical sculpture often suppresses it. The ideal athlete is not simply powerful. He is self-controlled. Emotionally disciplined. The body may be near maximum exertion, but the face refuses to surrender composure. It feels uncanny to modern viewers. Pliny criticized the lack of facial expression. Cicero wrote that “Myron’s works are not yet very close to the truth.”
The Discobolus doesn’t look like someone throwing a discus. He looks like the idea of controlled effort. I’m guessing that’s what Myron intended. This pose is deeply awkward in marble. The original bronze allowed limbs to extend freely into space. Thin structures are possible in bronze.
Marble is less forgiving. It wants support, and mass underneath the stress points. Roman sculptors adapting Greek bronzes had to add engineering solutions into the composition. Tree trunks, struts, and short connecting bridges. The damaged copy exposes more of that hidden problem. It looks slightly less like a perfect Platonic form and more like a negotiation with gravity.
We are taught to think of these sculptures as serene embodiments of timeless ideals, floating above ordinary technical concerns. But ancient sculptors were also engineers. They had to deal with leverage, fracture points, and concepts like center of mass.
A Roman copyist translating bronze into marble was solving a physics problem, and altering the sculpture in the process.
And we should clarify this idea of Roman copyists. By the imperial period, elite Roman culture was saturated with Greek art, Greek education, Greek teachers, Greek craftsmen. Many sculptors working in Rome were ethnically Greek, culturally Greek, or trained in Greek workshops and traditions. Some even signed their works with Greek names.
So when we say “Roman copy,” don’t imagine a guy in a toga photocopying ancient Greece. He might speak Greek, train in Athens, and sculpt Italian marble for a Roman patron.
“Roman copy of a Greek original” is misleading shorthand. By the imperial period, elite Greco-Roman culture was deeply entangled. Roman aristocrats consumed Greek art as cultural legitimacy. Entire chapters of Greek visual culture survive because wealthy Romans liked decorating their villas.
This all contributes to why art historians argue about copies. Every copy contains interpretation.
From different angles, this composition changes radically. One viewpoint produces clarity and balance. Another produces compressed confusion. Limbs overlap and his body seems almost tangled. Greek sculpture was increasingly designed for controlled viewing angles.
This Discobolus was discovered in 1781 on the Esquiline Hill. It emerged during the great age of aristocratic Roman collecting, when antiquities were prestige objects.
Like other classical sculptures, the Discobolus was recruited into political ideology. It was in the first load of artwork confiscated during Napoleon’s Italian campaign. Nazi aesthetics seized upon these athletic bodies as evidence of racial ideals, despite the obvious inconvenience that the sculpture was Greco-Roman.
Hitler personally admired the Lancellotti Discobolus. Hermann Göring purchased it in 1938 from Prince Lancelotti. It seems every era reinvents antiquity in its own image. The statue somehow survived.
See it in moving pictures:
History of Science in ‘A Canticle for Leibowitz’
Posted by Bill Storage in History of Christianity, History of Science on May 14, 2026
“Because a doubt is not a denial. Doubt is a powerful tool, and it should be applied to history.” – Thon Taddeo Pfardentrott
Walter Miller wrote the cyclical-apocalypse science fiction, A Canticle for Liebowitz, in 1959. Whoa. The novel’s structured in three major chunks spanning thousands of years. Despite the passage of time, each section mirrors the previous:
Fiat Voluntas Tua (Thy Will Be Done): Civilization reaches technological heights again. And repeats the original sin of hubris and annihilation.
Fiat Homo (Let There Be Man): Humanity struggles to recover lost knowledge after nuclear apocalypse.
Fiat Lux (Let There Be Light): Knowledge is rediscovered, science flourishes again, and, yeah, you know what happens. 1960 readers didn’t.
Humanity learns nothing that sticks through each cycle of apocalypse. The monks capture and retain some history but fail to understand. The Church’s continuity is the thread stretching through the cycles.
Monks preserve knowledge as relic. Sacred texts like blueprints and purchasing orders are copied and illuminated with zero knowledge of their meaning. Preservation gets ritualistic reverence. Monks maintain continuity, its content opaque. It echoes the pre-enlightenment attitude that the past is authoritative, and the best we can do is safeguard it.
The book is too long and complex for a guy like me to summarize and interpret. My goal is smaller and more particular. Miller obviously knows history of Christianity. He seems to know history of science well and he weaves epistemology into it.
He uses two characters, Brother Kornhoer the monk and Thon Taddeo Pfardentrott, a secular scholar. Kornhoer is a scientific-minded experimentalist, self-taught and deeply religious. He has a reverent awe toward natural phenomena. He invents an electrical dynamo and powers an arc lamp with it. Fellow monks deem it hellish.
Taddeo has immersed himself in electrical theory, which he is redeveloping, but has failed to demonstrate experimentally. He’s analytical, formal, and initially condescending to Kornhoer. Then seeing Kornhoer’s experimental progress, he praises him for his intuitive breakthroughs, commenting that it would have taken him, Taddeo, decades to discover this on his own.
Taddeo discusses Brother Kornhoer’s work with officials at the abbey:
“No, no, not the lamp. The lamp’s simple enough, once you got over the shock of seeing it really work. It should work. It would work on paper, assuming various undeterminables and guessing at some unavailable data. But the clean impetuous leap from the vague hypothesis to a working model—” Then thon coughed nervously. “It’s Kornhoer himself I don’t understand. That gadget—” he waggled a forefinger at the dynamo “—is a standing broad-jump across about twenty years of preliminary experimentation, starting with an understanding of the principles. Kornhoer just dispensed with the preliminaries. You believe in miraculous interventions? I don’t, but there you have a real case of it. Wagon wheels!” He laughed. “What could he do if he had a machine shop? I can’t understand what a man like that is doing cooped up in a monastery.”
On reading this, it hit me that Miller is quietly teaching History of Science. This is James Clerk Maxwell the theorist upon seeing the work of Michael Faraday, the self-taught, deeply religious experimenter associated with the Royal Institution – whose humility and faith mirrored the fictional monks’ values. And whose epistemic humility Maxwell took a lesson from.
Taddeo’s “wagon wheels!” exclamation is perfect. It grounds Kornhoer in practical mechanics rather than abstract scholarship. Faraday came from a bookbinder’s background and retained a craftsman’s relationship to apparatus. He manipulated coils, magnets, glass, wires. Maxwell then mathematized what Faraday felt.
Miller doesn’t name these references outright, but he seeds enough clues to suggest he’s fictionalizing them as archetypes of scientific discovery. This has to be common knowledge, I thought. Miller has put a a thin fictional veil on Faraday and Maxwell. Web searches find no discussion of the parallel.
Miller’s move here is shrewd. He’s not writing historical fiction per-se, but he’s dramatizing patterns from the history of science by pushing them into sci fi. Fiction as a tool for History of Science. (And here you’re supposed to understand that History of Science isn’t about names and dates.)
Miller has captured the tension between religious custodianship and scientific curiosity. He’s reminded us of the fragile transmission of pre-scientific knowledge through manuscripts and oral culture. He’s highlighted the way technological discovery (or recovery, here) precedes theoretical understanding (my Project Hail Mary review). He’s nailed the irony of having faith communities preserve secular knowledge better than secular institutions, especially post-catastrophe. The Jesuits, Aristotle’s Physics, and all that.
He’s hit on epistemology, that meeting of philosophy and science that genius nitwit scientists like Hawking and Dawkins are unable to grasp.
Maxwell deeply admired Faraday and treated his experimental insights as foundational. Though Faraday lacked formal mathematical training, his visual and experimental grasp of fields, lines of force, and induction profoundly shaped Maxwell’s work. Maxwell wrote:
“We are all, like Faraday, standing on the shoulders of giants, but the giant in this case is Faraday himself.”
More specifically, Maxwell’s 1856-65 work translating Faraday’s lines of force into a coherent mathematical model (culminating in Maxwell’s equations) was often accompanied by personal statements of humility and admiration. Maxwell saw his own equations as expressing Faraday’s intuitions in a generalized form, not as surpassing them.
In Canticle, Miller has distilled a real epistemological relationship: intuition feeds analysis, practice feeds theory. He dramatized it in a collapsed world where the expected roles are reversed. Instead of Cambridge and the Royal Institution, we get Kornhoer and Taddeo. One touches reality through experiment, another systematizes it. They recognize each other’s genius.
There’s another, less obvious, parallel. Taddeo’s reaction to Kornhoer also recalls Einstein’s attitude toward Georges Lemaître, a priest. Lemaître showed Einstein mathematically wrong. He derived an expanding universe. Einstein replied, “your calculations are correct, but your physics is abominable,” but was forced to concede.
Miller seems aware of a recurring pattern in the history of science. Posterity compresses the process of experimentation preceding theory into a clean but false narrative. He resists the “great linear progress” rational-reconstruction version of scientific progress and its history. In some ways, Miller preempted Feyerabend and Kuhn.
A final Feyerabendian point, which I don’t think I’m simply reading into Miller: “What’s a man like that doing cooped up in a monastery?” Miller undermines the modern belief that scientific brilliance belongs in institutions – secular or otherwise.
Taddeo questions the reliability of historical knowledge from the pre-apocalypse civilization. Someone challenges him along the lines of: if you doubt the old accounts, why study the ancient Leibowitz documents at all? Taddeo replies:
“Because a doubt is not a denial. Doubt is a powerful tool, and it should be applied to history.”
O Thick Wits, O Blind Watchers of the Sky
Posted by Bill Storage in History of Science on May 13, 2026
Everything changed right around the time of Johannes Kepler. Comets, against millennia of prior belief, were then discovered to be farther away than the moon. Aristotelian spheres had been shattered. Kepler’s Astronomia Nova announced his first two laws of planetary motion. 1: Planets moved in elliptical orbits. 2: Lines from the sun to each planet sweep out equal areas in equal times. Kepler’s deductions would have been impossible without the decades of meticulous data recorded by Tycho Brahe.
Then why was it Kepler who made these revelations, and not Tycho Brahe? The easy answer is that Johannes Kepler was a transcendent genius and Tycho Brahe was not. But that leaves out a bit that’s worth dissecting.
Brahe did something extraordinary. He made observational astronomy a precision science. Before him, astronomical measurements were uncertain by several arcminutes or worse. Tycho drove errors down toward a single arcminute. He used gigantic instruments, discipline, relentless correction and test/retest methodology. That sounds pedestrian compared to breaking Aristotle’s stronghold on thought, but it changed everything. Kepler later wrote that if Tycho’s data had been sloppier, circular orbits could have survived indefinitely.
The irony is that Tycho’s success probably trapped him intellectually. Tycho remained deeply committed to intuitive physics. Copernicanism didn’t feel right; the Earth obviously feels stationary. But his commitment was also because he took celestial physics seriously. If planets moved, what moved them? Why should Mars speed up and slow down? The Aristotelian-spheres model had indeed been cracked by the nova of 1572 and the comet of 1577. Tycho witnessed both of them. Yet, as a disciplined scholar, he wanted something mechanically intelligible in their place. His own geo-heliocentric system preserves much of the old psychological architecture: Earth central and stable, heavens ordered, motions essentially circular.
Kepler, who also initially resisted ellipses, was forced to face them. He became willing to sacrifice intuitive physics for mathematical truth. Radical. He spent years trying combinations of epicycles and ovals. The famous “eight minutes of arc” discrepancy in Mars’ orbit was decisive. Lesser minds would have dismissed it as measurement noise. For Kepler it was key. That required almost religious dedication to Tycho’s measurements.
Tycho grew up in a world where uniform circular motion was a metaphysical necessity. Circles were perfection, ellipses ugly. They seemed accidental and earthly. Kepler belonged to the transitional generation for whom reality had to fit observations.
There’s something familiar here. Scientific revolutions, as Thomas Kuhn saw them, often involve two different personalities who are incapable of understanding each other. One creates reliable phenomena, another reinterprets them. Tycho made planetary motion precise enough to become a problem. Kepler solved the problem by abandoning assumptions Tycho held sacred.
O crassa ingenia, O caecos coeli spectatores
“O thick wits, O blind watchers of the sky.”
Tycho wrote these words in the preface to De Nova Stella after the supernova of 1572. He hurled insults at scholars who refused to accept the implications of the “new star.” Aristotelian cosmology held the heavens to be changeless. Tycho measured the object carefully and showed it had no detectable parallax, meaning it was beyond the earth’s atmosphere. Aristotelian crystalline perfection was not.
Here is Tycho denouncing men who stare upward yet fail to see what is before them. Kepler later could have turned these words back on Tycho, who also stared directly at evidence having implications he refused to accept. His own measurements showed planetary motion was not circular, yet he remained committed to geometrically privileged circular motion.
Still, Tycho saw farther than his contemporaries. The subtlety here is easy to miss in “rational reconstruction” histories of science. Revolutionary evidence rarely announces its final meaning.
Tycho’s achievement was destructive before it was constructive. He demolished Aristotelianism with empirical rigor. That was enormous, and it happens often in science. The people who see anomalies often cannot reinterpret reality around them.
The tragedy and grandeur of transitional figures is that they can become prisoners of the conceptual worlds they destroy. Einstein is the obvious comparison. His work on light quanta brought the quantum revolution, yet he recoiled from indeterminacy and nonlocality: “God does not play dice.”
“Old fuddy-duddies” does not explain this. Einstein’s objections to quantum mechanics were profound and technically sophisticated. Tycho’s clutching a physically intelligible celestial order was not irrational.
Antoine Lavoisier and Lord Kelvin similarly opened doors they refused to pass through. We usually see Newton as immune to such reluctance. But consider: “That one body may act upon another at a distance through a vacuum… is to me so great an absurdity…” Sounds like Tycho.
Kepler and Bohr look prophetic in hindsight because history moved their way. Tycho lets us see the psychological cost of conceptual upheaval from the inside. Scientific revolutions are not merely logical sequences. They are struggles over what kinds of worlds some highly intelligent people can bear to inhabit while others cannot.
The Ugly Nero
Posted by Bill Storage in History of Art on April 1, 2026
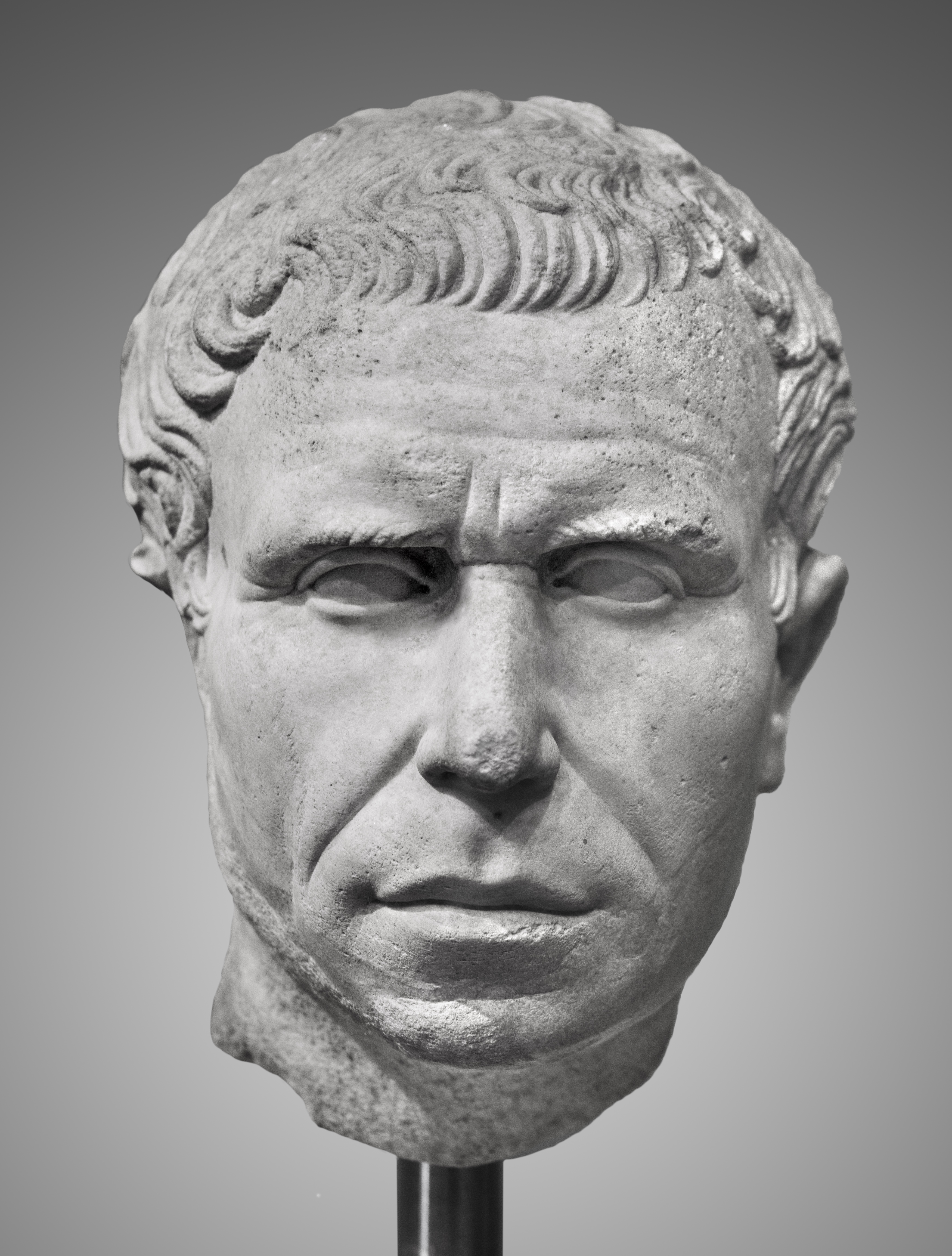
This is Nero, the infamous emperor who fiddled while Rome burned – or so the story goes – the story being a modern amplification of disreputable ancient sources.

This striking marble bust (Museo Capitolino inventory MC 0427) in the Capitoline Museums’ Hall of Emperors is one of the most photographed portraits of him. It’s certainly the ugliest. But there’s a twist.

Only this small upper part of the face is actually ancient. It probably originated as a portrait of Nero carved late in his reign, around AD 60 or later. After Nero was murdered, it appears the head was recarved in antiquity to represent Domitian instead.
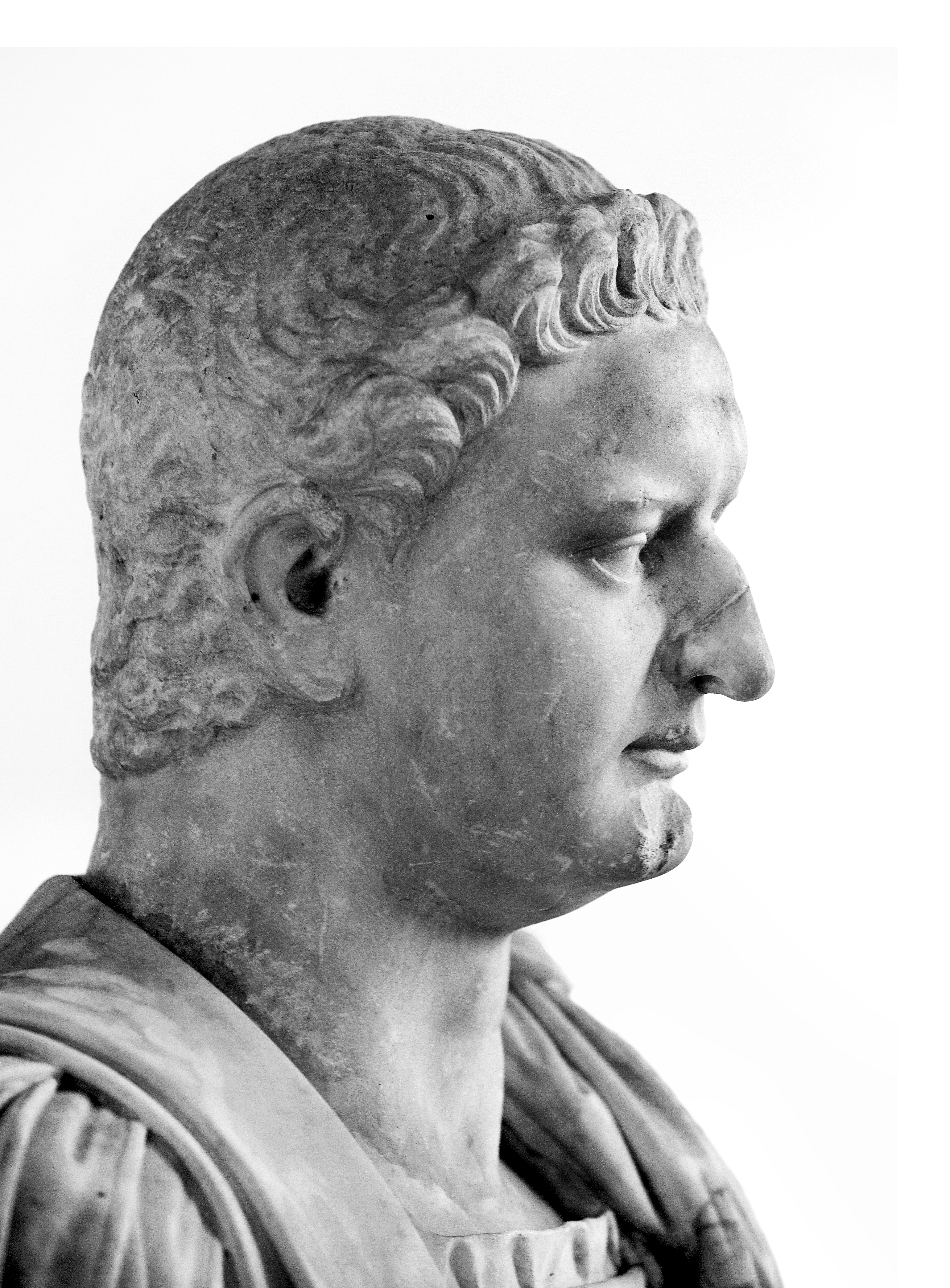
Some time later, it was damaged, leaving just the fragment highlighted here. Then, in the late 16th or early 17th century, Baroque restorers went to work for collectors like those in the Albani circle. The source of the original ancient head is unknown. It passed through the Giustiniani collection before entering the Albani collection, assembled by Cardinal Alessandro Albani in the 1700s. The Capitoline Museums acquired many pieces from the Albani collection in the 18th century as part of the museum’s early formation and expansion.
The Albacini workshop (Carlo Albacini and his son Filippo) was the cutting edge in Rome for restoring and completing ancient sculptures for collectors and the Grand Tour market. A drawing or related work by the Albacinis depicts “a fragment of Domitian restored as Nero,” suggesting their involvement. They completed almost the entire head, neck, and bust in the dramatic style of their time.
The result looks like Nero… Sort of. But compare it to better-preserved portraits of the real emperor and differences jump out. The proportions here are noticeably off – wider, coarser, perhaps deliberately unflattering.



The restored lower face and neck stand out sharply from Nero’s established types. We know this because we took detailed measurements of them and did statistical analyses.
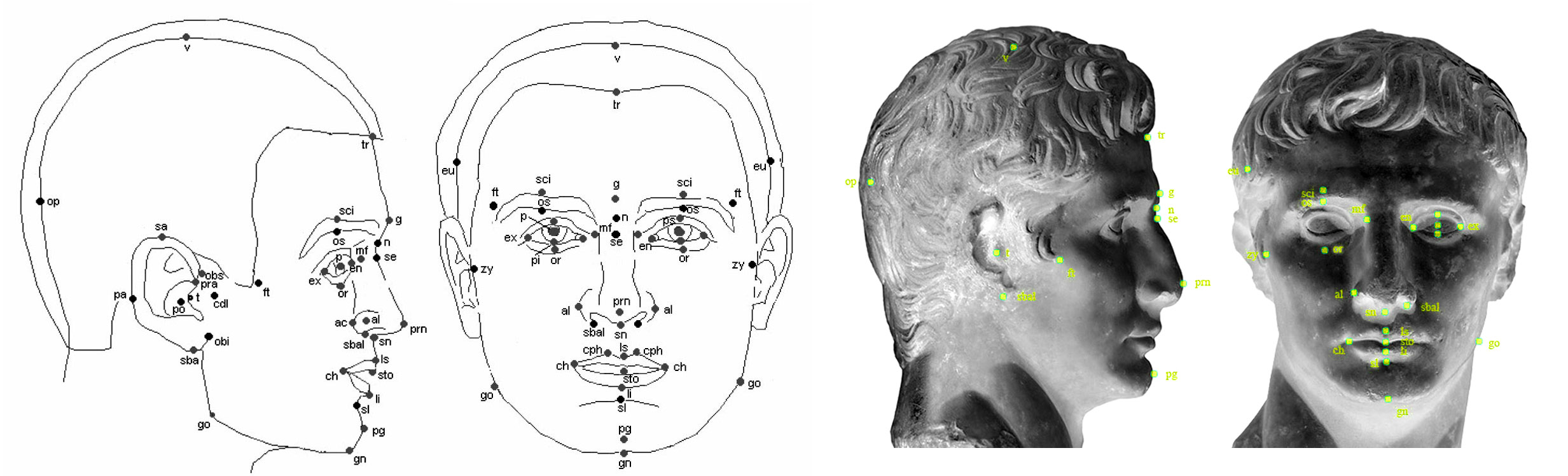
Why make Nero look almost hideous? It probably wasn’t ignorance. Other Nero portraits were known in Rome at the time. More likely, the restorers were channeling Suetonius, who described Nero as physically unappealing, with a thick neck and features that matched the image of a tyrant. Suetonius dies hard, even though we know he just made stuff up. Emperors, in ancient, Renaissance and modern minds alike, it seems, need to have been either great or terrible. Ancient physiognomy – the idea that looks reveal character – probably played a role in the restoration. They may have seen their job as more than just fixing marble. They were shaping a moral story.
This bust is a living record, layered with ancient politics, damage, and Renaissance imagination.
Next time you’re in the Hall of Emperors, look past the label. Roman portraits often tell us as much about the people who carved or restored them as about the emperors themselves.

—
See our YouTube short on this head of Nero
Anger As Argument – the Facebook Dividend
Posted by Bill Storage in Commentary, Ethics on January 16, 2026

1. Your partner has ordered the trolley conductor to drive away. If you order her to step out of the vehicle, and you briefly set foot on the track, you can repeatedly shoot her in the head and send the trolley careening out of control, possibly taking out another commie liberal, and the president will hail you as a hero. What do you do?
2. You’re at a crossroads and the only way to save your governor’s career and reputation is to take one for the team. Out of nowhere the frazzled ICE agent you’ve been threatening for days steps onto the trolley track. You can choose to sacrifice yourself in a final heroic act, slamming into that threat, keeping the governor safe and leaving your child an orphan. Do it now, or let Trump’s chaos reign. What’s your move?
The original trolley problems aimed at making you think. It was a philosophical puzzle used to explore moral reasoning, utilitarianism and deontology. Both versions above turn the trolley problem into a caricature. One paints federal force as the unstoppable threat that must be violently halted, the other paints civil disobedience as the lethal danger that must be neutralized. Each is designed to elicit tribal fervor.
These caricatures work on Facebook not because they clarify moral structure but because they flatter the reader and stage moral theater. The audiences already know who the villain is and get to enjoy the feeling of having seen through it all. Smug sarcasm supplies the laugh track.
What’s most depressing is the way such “humor” gets conscripted. Old fashioned wit punctured pretension and left everyone a bit exposed. This humor is ritualized sneer, a war cry that signals membership. Moral superiority and righteous indignation arrive prepackaged.
Whichever side you pick, your rage is justified. Anger becomes proof of righteousness. If I can mock you, I don’t need to understand you. If I can make others laugh at you, I don’t need to persuade them. Emotional reward comes first, the argument is decorative trim. I am furious. Therefore the offense must be enormous. My fury is not only justified but morally required. Anger stops being a response and becomes evidence. The hotter it burns, the stronger the proof. On Facebook this logic is amplified.
Philosophy, ethics, and moral reasoning slow things down. Facebook collapses time, context, and agency into a single cinematic moment. Pull the lever and cue the likes. Facebook rewards train people out of moral curiosity. Once sarcasm becomes the marker of insight, asking a genuine question is read as weakness. The platform punishes those who don’t escalate.
If something is free, the product is you. Facebook loves your self-justifying rage because rage compresses so well. A qualified objection is no match for indignation. Agreement becomes a reflex response. Once anger functions as proof, escalation is inevitable. Disagreement cannot be good faith. Arguments cease to be about the original claim and switch to the legitimacy of self-authenticating anger itself.
Facebook provides the perfect stage because it removes the costs that normally discipline rage. There’s no awkward pause, just instant feedback and dopamine.
To be taken seriously, you have to be outraged. You have to perform belief that the stakes are absolute. If your performance is good, you convince yourself. Likes makes right. Everything is existential. Restraint is complicity. The cycle continues. Facebook counts the clicks and sells them to Progressive Insurance, Apple, and Amazon.
___
Via Randall Munroe, xkcd
Robert Reich, Genius
Posted by Bill Storage in Commentary on December 25, 2025
Is Robert Reich a twit, or does he just play one for money on the internet?
I never cared about Monica Lewinsky. Bill Clinton was a big-picture sort of president, like Ronald Reagan, oddly. Flawed personally, but who are we to be critical? Marriage to Hillary might test anyone’s resolve with cigars and Big Macs. Yet somehow Clinton elevated Robert Reich to Secretary of Labor. Maybe he thought Panetta and Greenspan could keep the ideologue in check.
Reich later resigned and penned Locked in the Cabinet, a “memoir” devoured by left-wing academics despite its fabricated dialogues – proven mismatches with transcripts and C-SPAN tapes. Facts are optional when the narrative sings.
Fast-forward: Reich posted this on December 23:
“Around 70% of the U.S. economy depends on consumer spending. As wealth concentrates in the richest 10%, the rest of America can’t afford to buy enough to keep the economy running.”
Classic Reich: tidy slogan, profound vibe, zero nuance, preached to the CNN faithful.
Yes, consumption is ~70% of GDP. But accounting isn’t causation. Saying the economy “runs on” consumption is like saying a car runs on exhaust because that’s what comes out the back.
Wealth concentration doesn’t vanish spending:
- High earners save more per dollar, true – but they do spend (luxury, services) and, crucially, invest.
- Investment isn’t hoarded in vaults; it funds factories, tech, startups, real estate – creating jobs and future demand. U.S. history proves inequality and growth coexist.
- The economy isn’t a closed moral ecosystem: Government spending, exports, debt expansion, asset bubbles, and credit substitution all prop things up, sometimes for a long time and sometimes disastrously. Reich’s “can’t afford” is doing heroic rhetorical labor here.
Reich smuggles in a fixed “enough” consumption – for full employment? Asset bubbles? Entitlements? That’s the debate, not premise.
His real point is political: Extreme inequality risks instability in a consumption-heavy model. Fair to argue. But he serves it as revealed truth, as if Keynes himself chiseled it.
Reich champions “labor and farmers” while blaming Trump’s tariffs for the price of beef. Thank you Robert, but, as Deming argued (unsuccessfully) to US auto makers, some people will pay more for quality. Detroit disagreed, and Toyota cleaned their clocks. Yes, I’m willing to pay more for local beef. I’m sure Bill Clinton would, had he not gone all vegan on us. Moderation, Bill, like Groucho said about his cigar.
Reich’s got bumper-sticker economics. Feels good, thinks shallow.
Lawlessness Is a Choice, Bugliosi Style
Posted by Bill Storage in Commentary on December 8, 2025
Sloppiness is a choice. Miranda Devine’s essay, Lawlessness Is a Choice, in the October Imprimis is a furious and wordy indictment of progressive criminal-justice policies. Its central claim is valid enough: rising crime in Democratic cities is a deliberate ideological choice. Her piece has two fatal defects, at least from the perspective of a class I’m taking on on persuasive writing. Her piece is argued badly, written worse. Vincent Bugliosi, who prosecuted Charles Manson, comes to mind – specifically, the point made in Outrage, his book about the OJ Simpson trial. Throwing 100 points at the wall dares your opponent to knock down the three weakest, handing them an apparent victory over the entire case.
Devine repeats “lawlessness is a choice” until it sounds like a car alarm. She careens from New York bail reform to Venezuelan gangs to Antifa assassination. Anecdotes are piled on statistics piled on sarcasm until you’re buried under heap of steaming right-wing indignation.
Opponents are “nutty,” “deranged,” “unhinged,” or “turkeys who voted for Thanksgiving.” 20 to 25 million “imported criminals.” Marijuana is the harbinger of civilizational collapse. Blue-city prosecutors personally orchestrate subway assaults. Devine violates Bugliosi’s dictum throughout.
Easily shredded claims:
- Unsourced assertions of “20-25 million imported criminals.”
- Blanket opposition to marijuana decriminalization, conflating licensed dispensaries with open-air drug markets and public defecation as equally obvious “broken windows” offenses, even though two-thirds of Americans now support legal pot and several red states have thriving regulated markets.
- Stating that Antifa was plotting to assassinate Trump with no citation.
- Ignoring red-state violent-crime rates that sometimes exceed those of the blue cities she condemns.
A competent MSNBC segment producer – there may be one for all I know – could demolish the above in five minutes and then declare Devine’s whole law-and-order critique “conspiracy theory.” The stronger arguments – recidivism under New York’s bail reform, collapse of subway policing after 2020, the chilling effect of the Daniel Penny prosecution, the measurable crime drop after Trump’s 2025 D.C. National Guard deployment – are drowned in the noise.
The tragedy is that Devine is mostly right. Progressive reforms since 2020 (no-cash bail with no risk assessment, de facto decriminalization of shoplifting under $950, deliberate non-enforcement of quality-of-life offenses) have produced predictable disorder. The refusal of elite progressive voices to acknowledge personal agency is corrosive.
Bugliosi would choose his ground and his numbers carefully, conceding obvious points (red states have violent crime too), He wouldn’t be temped to merge every culture-war grievance. Devine chose poorly, and will persuade no one who matters. Now if Bugliosi had written it…
Ladies and gentlemen of the jury, the defense will tell you that crime spikes in American cities are complicated – poverty, guns, COVID, racism, underfunding. I lay out five undisputed facts, that in the years 2020–2024 major Democratic cities deliberately chose policies that produced disorder. They were warned. When the predicted outcome happened, they denied responsibility. That is not complexity but choice.
Count 1 – New York’s bail reform (2019–2020): The law eliminated cash bail for most misdemeanors and non-violent felonies, and required judges to release defendants with the “least restrictive” conditions. Funding was unchanged. Result: 2020-2023 saw over 10,000 rearrests of people released under the new law for new felonies while awaiting. In 2022 alone, at least 107 people released under bail reform were rearrested for murder or attempted murder. The legislature was warned. They passed it anyway. Choice.
Count 2 – Subway policing collapse: In January 2020 the NYPD had 2,500 uniformed officers assigned to the subway system. By late 2022 it was under 1,000. Felony assaults in the subway system rose 53 % from 2019 to 2023. This was deliberate de-policing ordered by City Hall and the Manhattan DA. Choice.
Count 3 – San Francisco’s Prop 47 and the $950 rule: California reclassified theft under $950 as a misdemeanor. Shoplifting reports in San Francisco rose 300%. Chain pharmacies closed 20 stores, citing unsustainable theft. The legislature refused every attempt to raise the threshold or mandate prosecution. Choice.
Count 4 – The Daniel Penny prosecution: Marine veteran Daniel Penny restrains a man who was screaming threats on a subway car. The man dies. Manhattan DA Alvin Bragg charges Penny with manslaughter. After two years of trial and massive expense, a jury acquits on the top count and deadlocks on the lesser; Bragg drops the case. Message sent: if you intervene to protect others, you roll the dice on court and possible prison. That chilling effect was the entire point of the prosecution. Choice.
Count 5 – The 2025 Washington, D.C. experiment: President Trump federalizes the D.C. National Guard and surges 3,000 troops plus federal agents into high-crime areas. Result in first 100 days: carjackings down 82%, homicides down 41%, robberies down 31% No gun buybacks – just enforcement. When the policy is reversed by court order, the numbers rose again within weeks. Enforcement works; the absence of enforcement is a choice.
Five exhibits, all public record. No unsourced 25-million-migrant claims, no Antifa conspiracy theories, nothing about Colorado potheads. Five policy decisions, five warnings ignored, five measurable explosions in disorder, and one rapid reversal when enforcement returned.
The defense will now tell you all about root causes. But I remind you that no city was forced to remove all consequences for criminal behavior. They were warned. They chose. They own the results. Lawlessness is a choice.
It’s the Losers Who Write History
Posted by Bill Storage in Commentary on November 24, 2025
The victors write first drafts. They get to seize archives, commission official chronicles, destroy inconvenient records, and shape the immediate public memory. Take Roman accounts of Carthage and Spanish on the Aztecs. What happens afterward and indefinitely is where Humanities departments play an outsized role in canonization.
Such academics are the relativist high priests of the safe-space seminary – tenured custodians of western-cultural suicide. Their scripture is the ever-shifting DEI bulletin. Credentialed barbarians stand behind at the gates they themselves dismantled. They are moral vacationers who turned the university into a daycare for perpetual adolescents. The new scholastic is the aristocracy of mediocrity. Historicist gravediggers have pronouncing the West dead so they can inherit its estate.
Several mechanisms make this possible. Academic historians, not primary sources – whether Cicero or Churchill – decide which questions are worth asking. Since the 1970s especially, new methodologies like social history, postcolonial studies, gender studies, and critical race theory have systematically shifted focus away from political, military, and diplomatic chronicling toward power structures, marginalized voices, and systemic oppression. These are not neutral shifts. They reflect the political priorities of the post-Nixon academic left, which has dominated western humanities departments since.
Peer-reviewed journals, university presses, hiring committees, and tenure standards are overwhelmingly controlled by scholars who share an ideological range scarcely wider than a breath. Studies of political self-identification among historians routinely show ratios of 20:1 or higher in favor of the left – often contented Marxists. Dissenting or traditional interpretations that challenge revisionist views on colonialism, the Soviet Union, or America’s founding are marginalized, denied publication, and labeled “problematic.” A career is erased overnight.
K-12 and undergraduate curricula worship academic consensus. Here, again, is a coherence theory of truth subjugating the correspondence model. When the consensus changes – when a critical mass of scholars finds an even more apologetic lens – textbooks follow, almost instantly. The portrayal of the European Age of Exploration, for example, went overnight from celebration of discovery to exclusive emphasis on conquest and genocide. American Founding Fathers went from flawed but visionary innovators of a unique government to rich slave-owning hypocrites, especially after the 1619 Project gained academic traction. A generation or two of Humanities college grads have no clue that “rich white man” Alexander Hamilton was born illegitimate in the Caribbean, was a lifelong unambiguous abolitionist, despised the slave-based Southern economic model, and died broke. They don’t know that the atheist Gouverneur Morris at the Constitutional Convention called slavery “a nefarious institution … the curse of heaven on the states where it prevailed.” They don’t know this because they’ve never heard of Gouverneur Morris, the author of the final draft of the Constitution. That’s because Ken Burns never mentions Morris in his histories. It doesn’t fit his caricature. Ken Burns is where intellectuals learn history. His The Vietnam War is assigned in thousands of high-school and college courses as authoritative history.
Modern historians openly admit that they mean their work to serve social justice goals. The past is mined for precedents, cautionary tales, or moral leverage rather than reconstructed for its own sake. The American Historical Association’s own statements have emphasized “reckoning with the past” in explicitly activist language. Howard Zinn (A People’s History of the United States) boasted, “I don’t pretend to be neutral.”
The academic elite – professional mourners at the funeral of the mind they themselves poisoned – have graduated an entire generation who believe Nixon escalated (if not started) the Vietnam War. This is a textbook (literally) case of the academic apparatus quietly rewriting the emphasis of history. Safe-space sommeliers surely have access to original historical data, but their sheep are too docile to demand primary sources. Instead, border patrollers of the settler-colonial imagination serve up moral panic by the pronoun to their trauma-informed flock.
The numbers. Troop levels went from 1000 when Kennedy took office to 184,000 in 1965 under Johnson. A year later they hit 385,000, and peaked at 543,000 when Nixon took office in 1969. Nixon’s actual policy was systematic de-escalation; he reduced US troops to 24,000 by early 1973, then withdrew the U.S. from ground combat in March. But widely used texts like The American Pageant, Nation of Nations, and Visions of America ignore Kennedy’s and Johnson’s role while framing Nixon as the primary villain of the war. And a large fraction of the therapeutic sheep with Che Guevara posters in their dorms graze contentedly inside an electric fence of approved opinions. They genuinely believe Nixon started Vietnam, and they’re happy with that belief.
If Allan Bloom – the liberal Democrat author of The Closing of the American Mind (1987) – were somehow resurrected in 2025 and lived through the Great Awokening, I suspect he’d swing pretty far into the counter-revolutionary space of Victor Davis Hanson. He’d scorch the vanguardist curators of the neopuritan archival gaze and their pronoun-pious lambs who bleat “decolonize” while paying $100K a year to be colonized by the university’s endowment.
Ken Burns said he sees cuts to the Corporation for Public Broadcasting as a serious existential threat. He did. The republic – which he calls a democracy – is oh so fragile. He speaks as though he alone has been appointed to heal America’s soul. It’s the same sacerdotal NPR manner that Bloom skewered in the humanities professoriate: the priestly conviction that one is engaged in something higher than mere scholarship, something redemptive. And the nation keeps paying Burns for it, because it’s so much more comfortable to cry over a Burns film than to wrestle with the actual complexity Burns quietly edits out. He’s not a historian. He’s the high priest of the officially sanctioned memory palace. It’s losers like Burns who write history.
Things to See in Palazzo Massimo
Posted by Bill Storage in History of Art, History of Christianity on November 10, 2025
Mike and Andrea visit Rome this week. Here’s what I think they should see in Museo Nazionale Romano, Palazzo Massimo. Not that I’d try to push my taste on anyone.
The Via Labicana Augustus
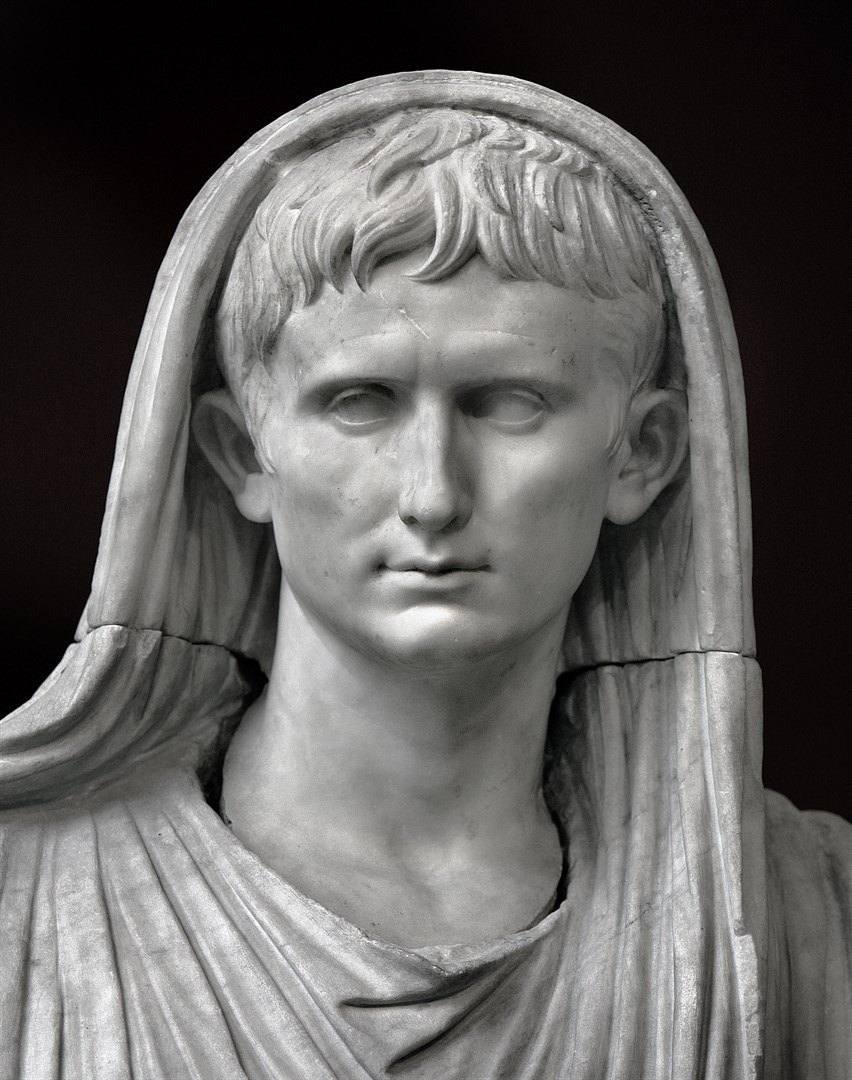
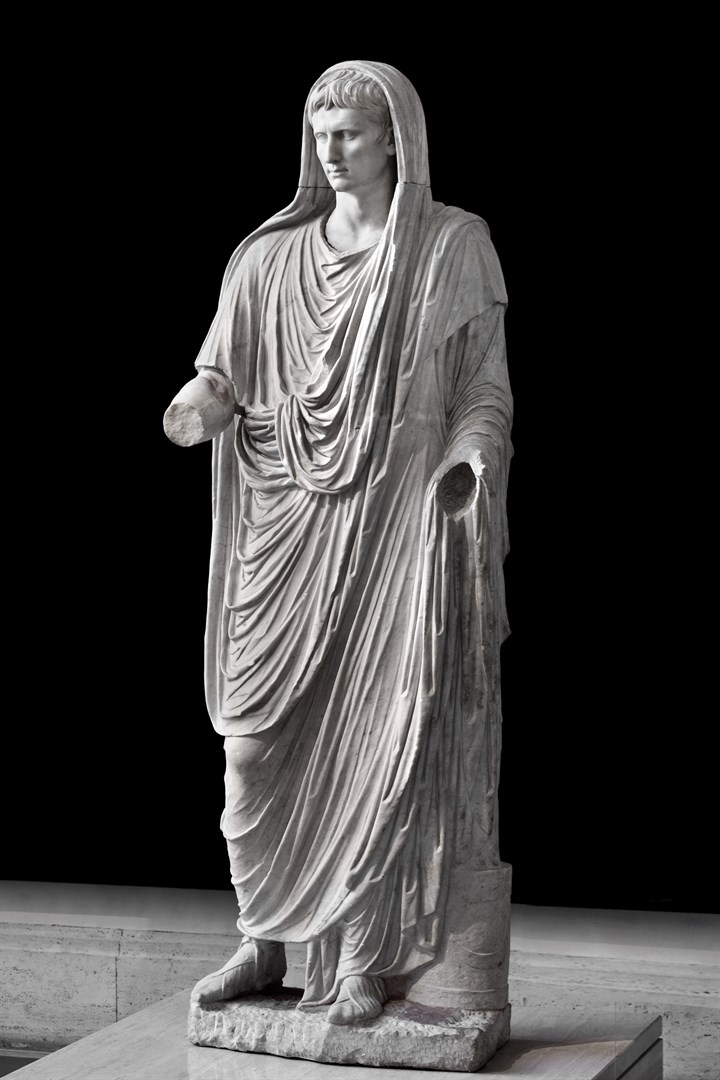
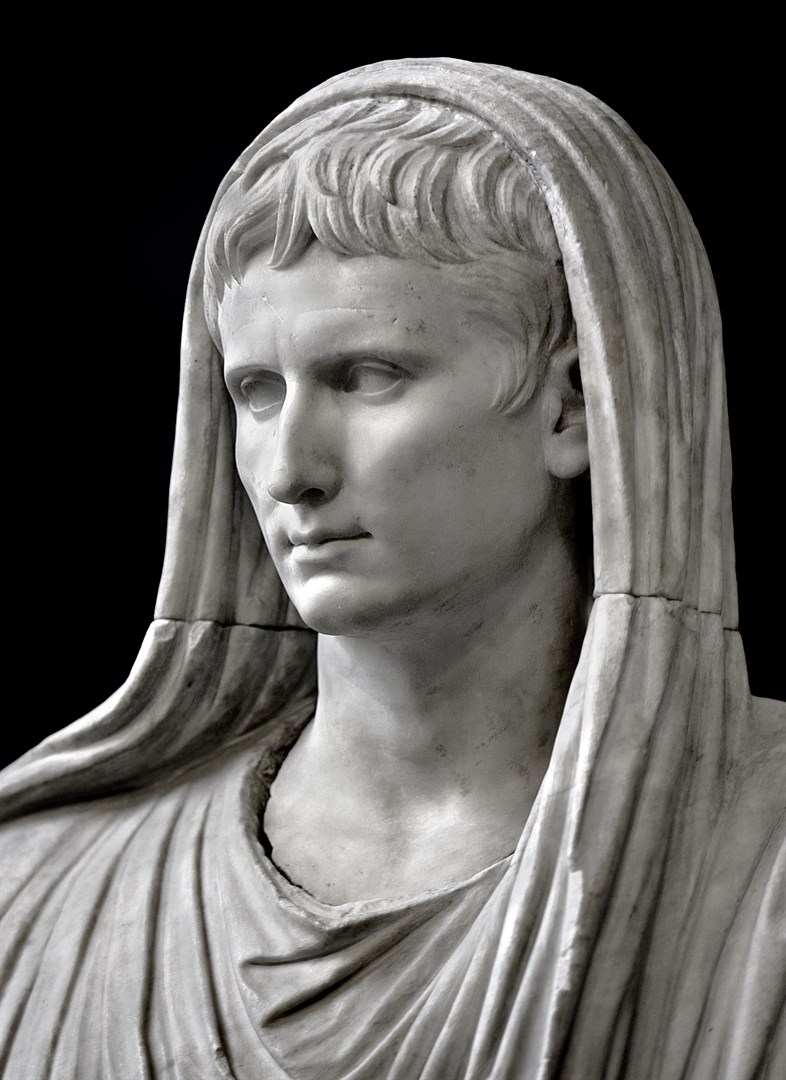
The Via Labicana Augustus was discovered in 1910 near the Via Labicana, southeast of Rome. It probably dates to 12 BCE, the year Augustus became Pontifex Maximus, chief priest of Rome.
The statue shows him veiled, performing a sacrifice, wearing the toga pulled over his head in the ritual gesture known as capite velato. Unlike the heroic, idealized Augustus of Prima Porta, this image presents him not as a godlike conqueror but as the pious restorer of Rome’s religious traditions. The face retains a calm, idealized realism – a softened continuation of late Republican verism – while the body’s smooth drapery and composed stance convey dignity and divine favor.
The piece reveals Augustus’s political strategy of merging personal authority with religious legitimacy. By showing himself as priest rather than warrior, he presented his rule as moral renewal and continuity with the Republic’s sacred traditions, rather than naked monarchy.
The Portonaccio Sarcophagus



The Portonaccio Sarcophagus, carved in high relief around 180-190 CE, is one of the most elaborate Roman sarcophagi from the late second century CE. It was discovered in a tomb in 1931 near the ancient Via Tiburtina in the Portonaccio area of Rome.
The front is a dense, chaotic battle scene. Roman soldiers clash with barbarians in a tangle of limbs, shields, and horses. There’s no clear spatial depth, just a frenzied mass of combat, carved almost in relief upon relief. At the center stands the Roman general, larger and calmer than the rest, commanding order amid chaos. His face is idealized, yet individualized; his bare head suggests he may have died before receiving a victory crown.
This style marks a shift from the classical order of earlier art to the expressive, almost abstract energy of late imperial sculpture. It reflects the constant warfare and political instability of the era. It likely commemorated General Aulus Iulius Pompilius, who served under Marcus Aurelius.
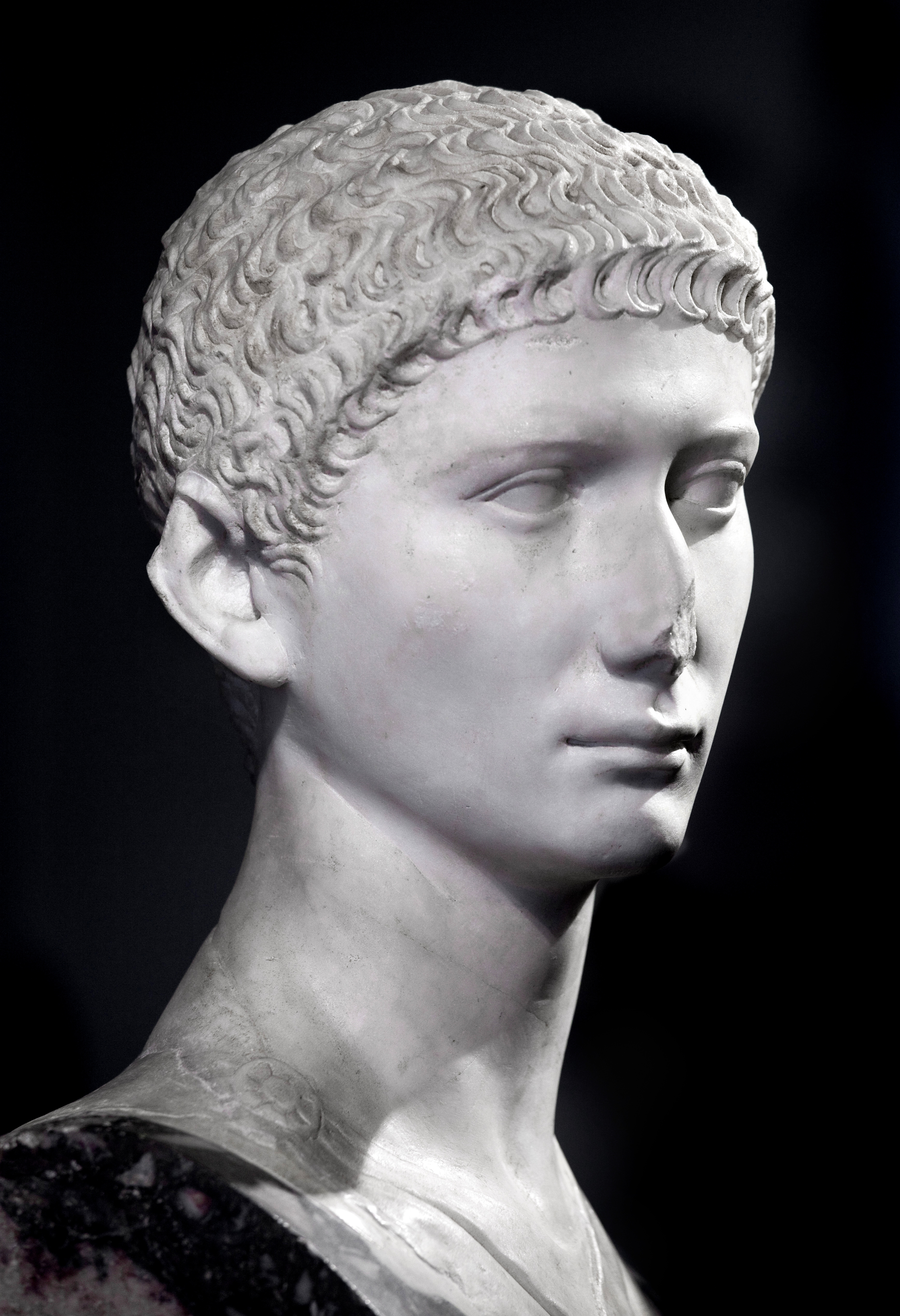
Colossal Bust of Gordian III

The colossal marble bust of Gordian III presents a striking – if not bizarre – image of the boy-emperor struggling to embody imperial gravitas. Created around AD 244, it reflects the tension between youthful vulnerability and the formal ideals of Roman authority.
Gordian III came to the throne after a cascade of assassinations during the “Year of the Six Emperors.” The sculptor has rendered him with the smooth, unlined face of an adolescent, but framed by the austere, hieratic composition typical of imperial portraiture – short military haircut, heavy-lidded eyes gazing slightly upward, and a thick neck suggesting strength he did could not have possessed. The result is almost tragic: the image insists on imperial permanence while hinting at fragility.
Stylistically, the bust belongs to the late Severan, early soldier-emperor phase, where portraiture shifts from the individualized realism of the Antonines to a more schematic, abstract treatment of features. The deep drilling of the hair and the intense, static expression anticipate the hard linearity of third-century imperial art.
The Charioteers





The charioteer portrait busts date from the early fourth century CE and depict professional aurigae – chariot racers who were the sports celebrities of late imperial Rome.
These busts show men with distinctive attributes of their trade: short, tightly curled hair, intense gazes, and tunics bound with leather straps across the chest, used to secure their protective harnesses during races. The faces are individualized, confident, and slightly idealized, conveying both athletic vigor and the proud self-awareness of public fame.
They likely commemorated successful drivers from the great Roman circuses, perhaps freedmen who had risen to wealth and status through racing. The style, with its crisp carving and alert expression, reflects late Roman portraiture’s mix of realism and formal abstraction – an art no longer concerned with classical balance, but with projecting charisma and presence.
Republicans
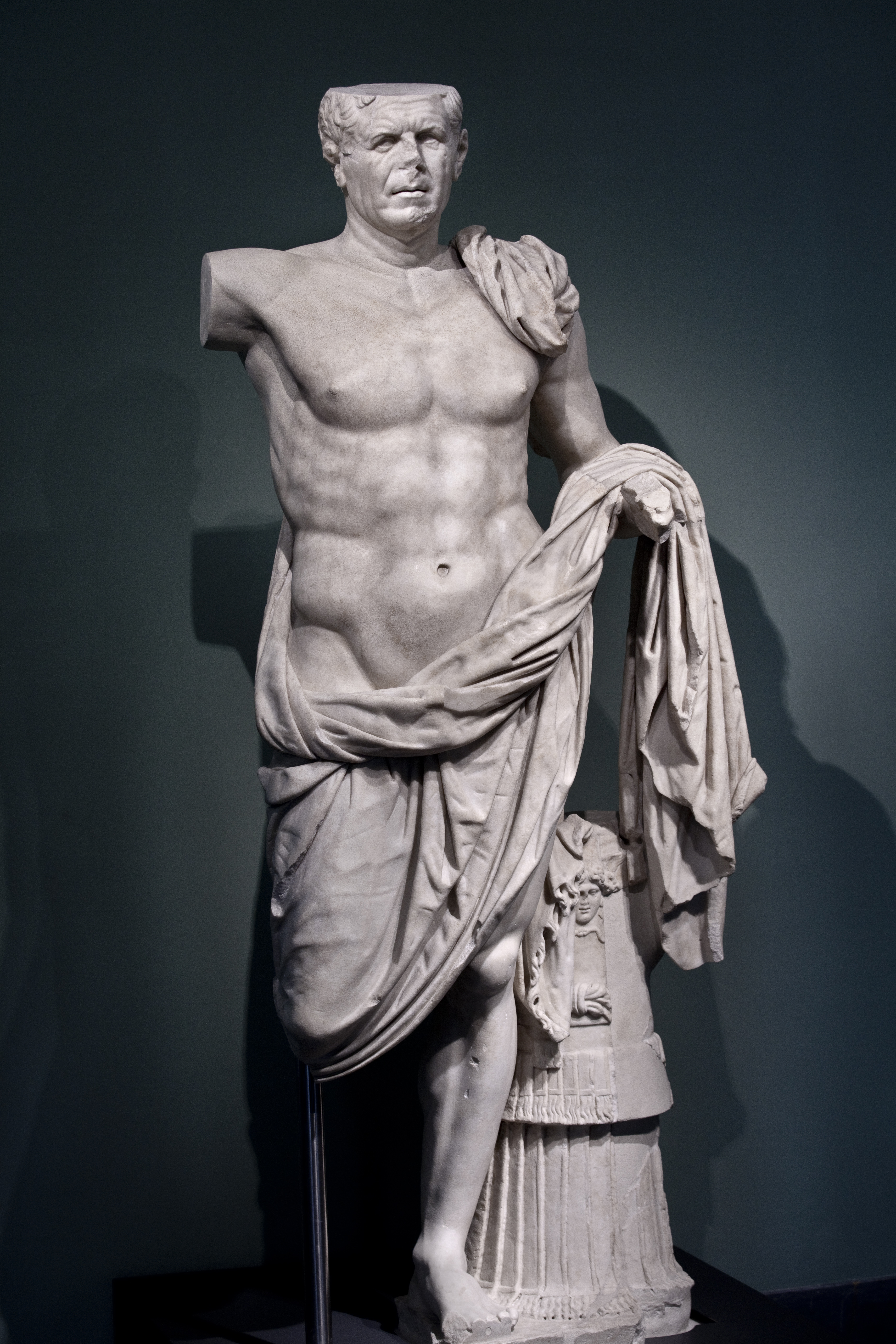
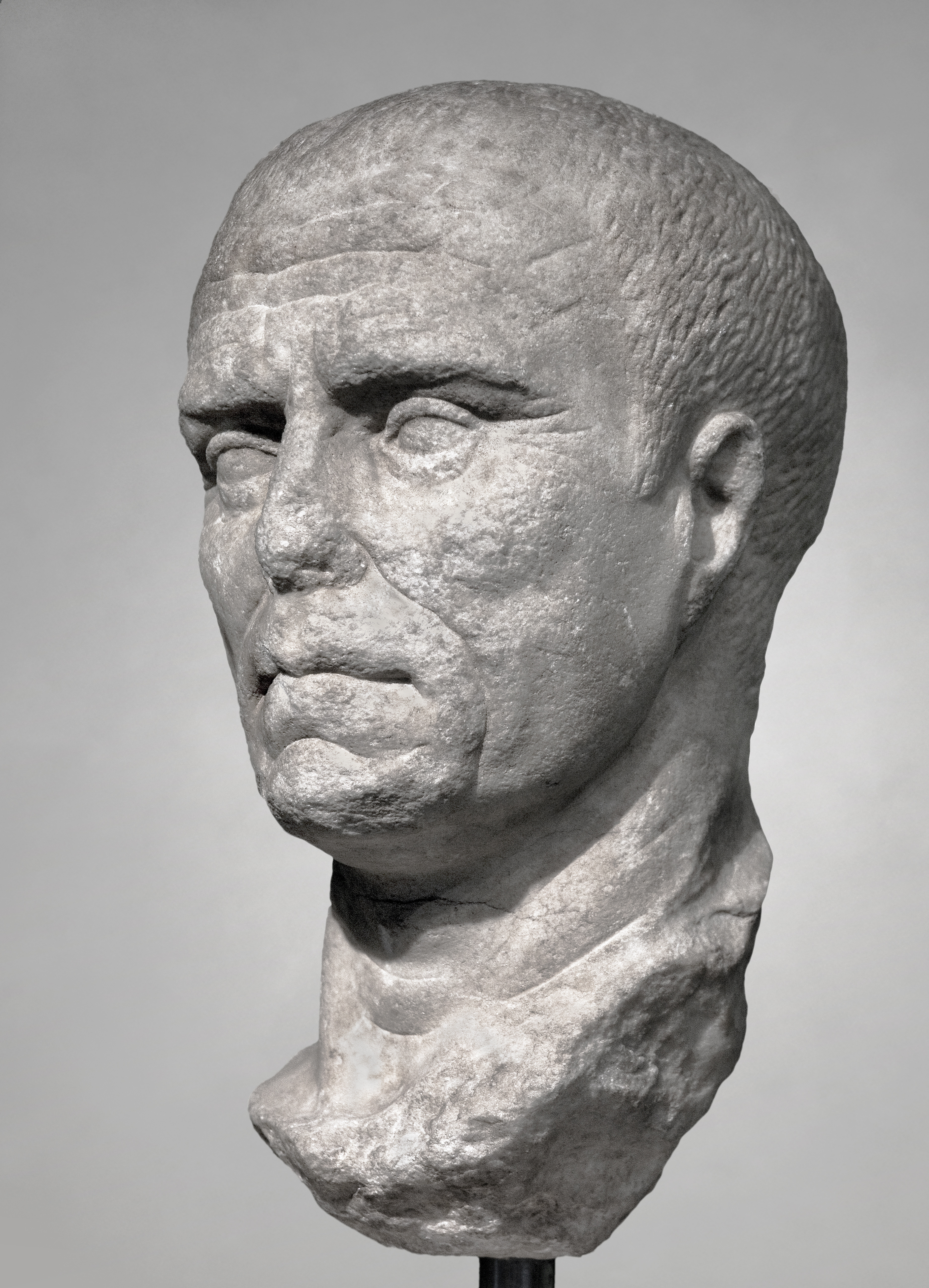



The so-called General from Tivoli (Terme inv. 106513) was found beneath the Temple of Hercules in 1925. Dating to about 70 – 90 BC, he was probably a lieutenant of Sulla. The late-Republican portrait busts (Inv. 112301 and 114759) are famous for their verism – a style emphasizing unidealized realism. Rather than the smooth, youthful perfection of Greek sculpture, Roman patrons in this period wanted faces that looked weathered and unmistakably mortal. Eyes were often sharply undercut and hollowed to give depth and intensity. Cheeks could appear gaunt, lips thin and compressed, necks stringy. The overall effect was one of disciplined austerity and civic virtue – a face hardened by service to the Republic.
The young woman’s elaborate hairstyle (inv. 125591, just above) is a social signal, suggesting she belonged to a wealthy family or wanted to look the part. The combination of a classicizing ideal face with a detailed fashionable hairstyle suggests a woman who wants to present both grace and her social status. That blend of realism and idealization is typical of the late republic.


This was more selective exaggeration than realism. These men were advertising moral qualities: gravitas, virtus, fides. By the time of Caesar, you see a blending of this verism with a hint of idealization, anticipating the smooth, godlike Augustan portraits to come.
Speaking of late Republicans, this marble portrait of an elderly woman with her hair in a bun brings to mind another later Republican – Ronald Reagan.
The Sarcophagus of Marcus Claudianus

The continuous-frieze sarcophagus of Marcus Claudianus shows New Testament scenes on its front; and New and Old Testament scenes on its lid, along with pagan elements. The grape harvest imagery on the lid is ambiguous; it appears on pagan and Christian sarcophagi with identical elements. From left to right on the lid: Jesus nativity scene, sacrifice of Isaac, inscription naming the deceased, image of the deceased as scholar, grape harvest scene.
Carvings on the front of the sarcophagus: Arrest of Peter (Acts 12:3), miracle of water and wine (with possible baptism reference, John 2:1), orant figure, miracle of loaves (Mark 6:30–44, Matt 14:13–21, Luke 9:10–17, John 6:1–14), healing a man born blind (John 9:1), prediction of Peter’s denial (Mark 14:27–31, Matt 26:30–35, Luke 22:31–34, John 13:36–38), resurrection of Lazarus (John 11:1), and supplication of Lazarus’s sister (John 11:32).
The scenes on this sarcophagus include several apparent departures from scriptural miracle stories. Jesus appears in three places as magician, using a wand to perform miracles. He stands above five baskets of bread, a number consistent with most sarcophagi of its age but inconsistent with either of the loaves-and-fish scriptural pairs, where the remaining baskets number seven and twelve (Matthew 4:17, Matthew 15:34). This could have been a choice made by the sculptor for purely artistic reasons. The orant figure in the center is similar to those seen on earlier gravestones, and does not seem to be a scriptural reference. This posture is similar to that of the three youths in the furnace and the common sarcophagus scene of Jesus passing the new law to Peter and Paul (non-scriptural).
The Marcus Claudianus sarcophagus stands out for the prominence of Johannine-only imagery – Lazarus, the man born blind, Cana – scenes that are either uniquely Johannine or given distinct theological weight in that gospel. I don’t think you’ll hear this from anyone but me. I love this sarc for this reason. Compared to the sarcophagi from the Vatican necropolis, whose iconography often centers on synoptic or composite miracle cycles (feeding, healing, Jonah, Daniel, Good Shepherd), this sarc shows a notable shift toward Christological revelation rather than simple miracle narrative.
That shift says to me: mid-4th-century context, when Johannine motifs had become the backbone of Christian funerary theology. By that time, art was turning from generic symbols of deliverance to narratives that expressed Christ as Logos and life-giver, echoing themes prominent in the theological debates of the post-Nicene generation. The Lazarus scene, for example, takes on explicit resurrection connotations, and the healing of the blind man becomes an emblem of illumination through baptism – precisely the kind of allegorical reading developed in the decades after Constantine.
Earlier dating has been given by some scholars. Bunk. That impulse reflects anxiety over the scarcity of securely dated pre-Constantinian Christian monuments in Rome. Stylistically and iconographically, the Claudianus piece sits more naturally with sarcophagi of the 340s-360s: compressed compositions, monumental heads, frontal orant, and a selective, theological rather than narrative use of miracle scenes. And that’s probably more than you wanted to know about a topic I find fascinating because of what it says about modern Catholicism.
Bronze Athletes





The bronze athletes date from the Hellenistic period (second to first century BCE) convey the victory, exhaustion and fleeting nature of athletic glory.
The most famous of them, the Terme Boxer, was discovered on the Quirinal Hill in 1885. He sits slumped, body still powerful but spent, his face swollen and scarred, his hands wrapped in leather thongs. The artist cast every cut and bruise in bronze, even inlaid copper to suggest blood and wounds. Yet his expression is not defeat but endurance – a man who’s given everything to the arena.
Nearby, the Hellenistic Prince (or Terme Ruler), found in the same area, stands upright and nude, the counterpart to the seated boxer. His stance is heroic but weary, his gaze detached. Together the two figures tell both a moral story and a physical one: the the beauty and cost of strength.
These bronzes were likely imported to Rome as prized Greek originals or high-quality copies for a wealthy patron’s villa. They embody the Greek ideal of athletic excellence reframed through Roman admiration for the discipline and suffering behind it.
Wall Paintings/Frescoes

The villa wall paintings in Palazzo Massimo form one of the richest surviving narratives of Roman domestic life and taste. Most come from suburban villas around Rome, dating from the late Republic through the early Empire, and they recreate the visual world of elite Roman interiors.
The centerpiece is the set from Livia’s Villa at Prima Porta, discovered in 1863. The walls depict an illusionistic garden in full bloom – fruit trees, flowers, birds, and a soft blue sky.




Other rooms, such as those from the Villa of Farnesina, show mythological scenes, architectural vistas, and richly colored panels framed by columns and imaginary shrines. These follow the Second and Third Styles of Roman wall painting: first creating deep, theatrical perspective, then shifting to flatter, more decorative compositions filled with miniature landscapes and floating figures.
Taken together, the frescoes chart Rome’s transition from the austere republican taste for illusionistic space and Greek motifs to the sophisticated imperial language of myth, luxury, and controlled fantasy.
Cristo Docente



The Cristo Docente (Teaching Christ) clearly shows a youthful, androgynous body with small breasts. This is visual language flowing directly from Greco-Roman conventions of the philosopher, ephebe, or Apollo rather than an ethnographically accurate depiction of any historical Jesus. This one of the earliest depictions of Jesus, and a very rare example of Christian art not associated with burial. I wonder what the Vatican would trade for it.
Early Christian artists weren’t attempting realism; they were translating abstract theological ideas into iconic forms the viewer would recognize. The effeminate traits signal spiritual rather than biological qualities – gentleness, wisdom, eternal youth – while the frontal, often seated or teaching pose evokes authority and composure. In that cultural moment, a physically idealized, effeminate figure would convey the moral and divine authority expected of a teacher or savior without challenging Roman notions of masculinity, which were more flexible in the context of idealized youth and divinity.
The Christian anxiety that arises from this piece crack me up. Modern viewers, steeped in historical or doctrinal literalism, try to read the image literally. That’s a projection: the image is a theological construction, not an ethnographic one. Christian art critics, especially in the early 20th century, bristled at the iconography and tried to brush the thing off as a young girl posing as a scholar, rather than relaxing into the idea that early Christians weren’t like them.
The Discobulus
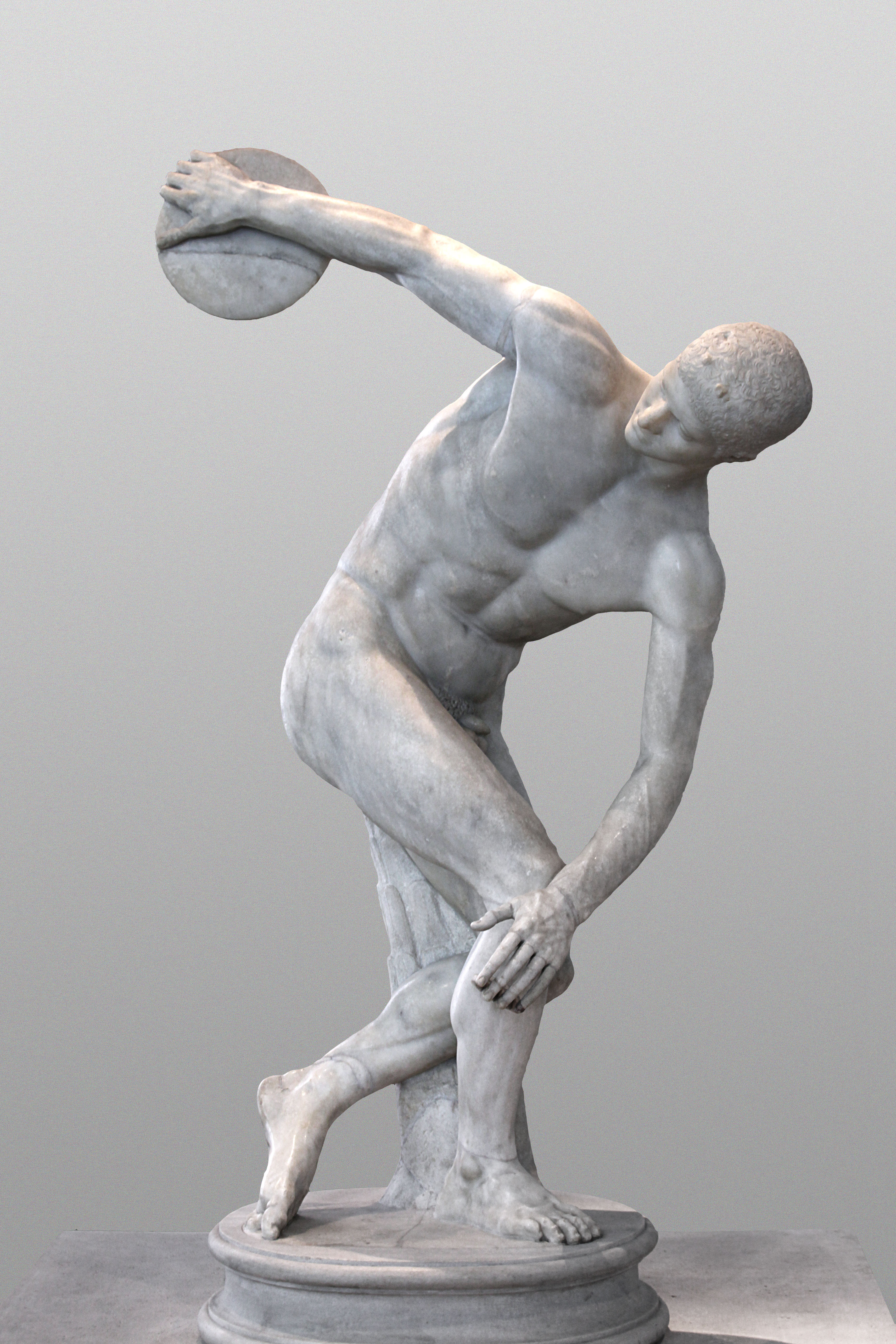
This discobolus is interesting because it’s a Roman copy of a Greek original (traditionally attributed to Myron, mid-5th century BCE) but reinterpreted in a Roman context. Several points stand out:
Roman taste for idealized athleticism – Unlike the athletes that highlight strain and fatigue, the Discobolus captures frozen, perfect form in mid-action, emphasizing harmony, proportion, and controlled energy. The figure is taut, but serene, a demonstration of mastery over both body and motion.
Technical virtuosity – The sculpture compresses a dynamic twist of the torso and rotation of limbs into a balanced composition. The Massimo copy preserves this elegance while subtly softening the muscular definition compared with Hellenistic copies that exaggerate tension.
Cultural resonance in Rome – Displaying this statue in a Roman villa or public space signaled the moral and civic ideals associated with disciplined youth, athletic virtue, and controlled action—qualities the Roman elite wanted to project.
Roman copy as a lens on reception – we see how Romans interpreted Greek originals, choosing what to preserve, emphasize, or downplay. Unlike more dramatic Hellenistic works, this Discobolus shows restraint, aligning with Roman preferences for clarity, proportion, and intelligibility over theatricality. It’s a visual bridge between Greek athletic ideal and Roman moral-aesthetic ideology.
Bronze from Caligula’s Ships


The bronze fittings come from the two grand ceremonial vessels built in the lake of Lake Nemi, ordered by Gaius Caligula around AD 37-41. By commissioning such a floating palace, Caligula aligned himself with Hellenistic kings and with the mastery of nature. The bronzes speak that language of luxury and sacerdotal authority.
The vessels and their fittings were masterpieces of maritime technology, supported by massive beams, outriggers, twin rudders, and elaborate decoration. The bronze protomes were integrated in the structural and mechanical system of the ship (rudders, beams, mooring rings). Here is the transition from Republic to Imperial ornamentation in full flourish – Roman taste for Hellenistic luxury, combined with native iconography. The bronzes bridge functional object, architectural ornament, and political symbol.

Republicans Against Democracy
Posted by Bill Storage in Commentary on April 9, 2026
The aim of protest is to misrepresent the proportion of people holding a given opinion by being more conspicuous than those not holding that view.
You might argue, in response, that protest is less about measuring opinion than “signaling intensity.” Ten thousand mildly supportive people and five hundred highly motivated people are not equivalent in political terms, you might say. The latter will donate, organize, vote in primaries, and make life difficult for officials. Protest is a way of saying, “we care enough to incur cost.” That’s information, says the organizer.
Then maybe you’ve made my point. In a democracy – democratic republic, more correctly – someone in that highly motivated group should still cast but one vote.
A protest and its media coverage create the impression of a groundswell that isn’t there. And there’s a continuity between “signaling intensity” and “nudging conformity.” Social visibility tells folk seeking peer approval “this is the crowd to be part of.”
If a protest makes a stance feel socially legible and non-isolating, it lowers the cost of adopting it. Deep-pocket funding can tilt who gets organized and which messages are polished. It can lower barriers for certain groups, provide stipends for organizers, and shape the tone of events. That can make a movement look more coherent or widespread than it would be if people had to self-organize, like they did in 1967.
Media bias, including social media hosted by big concerns like Facebook, X and Google, is an obvious source of concern. Case in point: Google’s apparent attempt to coerce me right here. I intended to call this essay “Democrats Against Democracy.” So I asked Google Gemini to make me an image of an angry man holding a sign saying “Democrats against democracy.”
It refused. I asked two more times, using different language. It instead built me an image of a man holding a sign reading “Democrats against corruption.” So I then asked for an angry man with “Republicans against democracy.” Thank you.
I cover a wide variety of topics on this blog. From my WordPress stats, I can conclude that textual analysis of the Gospel of Mark and stress analysis of concrete expansion bolts are hotter topics than politics. I can’t know for sure whether Google suppresses my political posts, but it seems curious that Mark and concrete bolts each got 40 times as many views as my pieces criticizing covid response. 40 times.
Elections confer authority, they shouldn’t suspend dissent. Protest can be a normal part of democratic feedback when it tries to change minds or set agendas. It can be clearly anti-democratic when it aims to nullify lawful outcomes or intimidate participation. Help me draw the line?
Watch my short video spoof about Careers in the Protest Economy on YouTube. YouTube is owned by Google. This video got one fiftieth as many views as the one I made about a particular marble bust of emperor Nero a day later. Timely topic, Nero.
democracy, history, news, politics, trump
1 Comment